'%3e%3cpath%20d='M136%2043.0521C135.893%2043.4991%20131.298%2041.3697%20123.51%2041.5186C120.787%2041.5712%20109.626%2040.8001%20104.06%2049.4228C101.316%2053.664%20102.266%2056.2491%20100.601%2061.5769C95.2065%2078.8661%2087.7394%2075.1856%2062.5302%2088.5228C54.5058%2092.764%2045.1595%20101.562%2043.5589%20103.087C31.9403%20114.163%2025.1664%20123.189%2025.1521%20123.171C25.1378%20123.162%2034.1912%20104.357%2047.7676%2082.7655C60.6795%2062.2429%2063.8235%2070.0769%2079.7722%2049.1336C81.7015%2046.6011%2084.8526%2037.6805%2089.683%2036.1032C93.6345%2034.815%2098.6148%2036.6114%20100.065%2038.5568C101.044%2039.8712%20101.459%2040.765%20103.831%2040.4408C110.048%2039.5996%20113.613%2039.8625%20115.492%2039.7748C116.95%2039.7047%20119.751%2039.915%20120.509%2039.9939C130.419%2040.9753%20136.15%2042.4563%20136.007%2043.0434L136%2043.0521Z'%20fill='%23127398'/%3e%3cpath%20d='M22.1867%2043.6392C30.3968%2055.0923%2031.5544%2062.348%2040.6506%2068.6923C45.9954%2072.4253%2053.4839%2075.4134%2058.2928%2075.5361C61.9084%2075.6325%2063.7305%2075.2557%2064.6023%2074.949C64.8524%2074.8614%2065.1025%2074.8351%2065.3597%2074.8263L76.0636%2070.6727C76.8068%2066.8871%2076.1637%2063.4784%2076.1065%2063.1892C75.0561%2058.0103%2072.3337%2053.3835%2070.5402%2051.2542C55.4561%2033.3428%2055.8062%2034.298%2046.5814%2028.0237C26.7884%2014.5902%20-1.22192%2021.3464%200.0428309%2022.0562C0.55016%2022.3454%2010.2394%2026.9634%2022.1867%2043.6392Z'%20fill='%23127398'/%3e%3cpath%20d='M79.8366%2044.0161C81.33%2046.4784%2083.4093%2051.5784%2083.7666%2056.8975C83.7952%2057.3094%2084.1667%2064.0393%2080.4654%2068.4733C78.5004%2070.8217%2076.2281%2071.5403%2075.585%2071.7506C61.487%2076.5264%2028.4319%20116.196%2023.3515%20133.494C23.2229%20133.941%2022.6227%20136.026%2022.5655%20136C22.3797%20135.921%2023.5373%20120.753%2028.925%20106.303C28.925%20106.303%2033.7196%2090.5295%2046.7387%2073.9326C49.1896%2070.8042%2052.8052%2067.0362%2052.8052%2067.0362C54.2414%2065.1434%2059.8006%2068.3068%2066.1887%2068.482C69.9401%2068.5872%2073.2198%2067.6846%2073.2055%2067.3604C73.2055%2067.2377%2073.0698%2067.0712%2072.8911%2066.9047C72.3195%2066.3702%2071.5907%2066.1423%2070.8761%2066.2475C69.9758%2066.379%2068.1323%2066.3877%2064.5738%2065.5903C59.8435%2064.5212%2052.8481%2060.096%2048.0534%2055.364C39.9076%2047.3109%2039.7147%2039.9238%2033.1051%2026.9985C23.4944%208.17586%2014.0767%201.32328%2014.0767%201.32328C17.285%20-1.64734%2041.451%20-0.788575%2059.229%2016.3692C67.5177%2024.3697%2067.2962%2023.3619%2079.8366%2044.0073V44.0161Z'%20fill='%23EF9920'/%3e%3c/g%3e%3cdefs%3e%3cclipPath%20id='clip0_882_3310'%3e%3crect%20width='136'%20height='136'%20fill='white'/%3e%3c/clipPath%3e%3c/defs%3e%3c/svg%3e)
Long-Term Care (LTC)
What It Costs, What Medicare Won't Cover, and the Mistakes That Leave Families Financially Exposed
Long-term care (LTC) refers to ongoing assistance with the basic activities of daily living — bathing, dressing, eating, toileting, continence, and transferring (moving from bed to chair) — or supervision required by cognitive impairment such as dementia or Alzheimer's disease. It is not medical treatment in the traditional sense. A hospital fixes an acute problem; long-term care supports someone who can no longer fully care for themselves over an extended period, often years or decades.
The Department of Health and Human Services estimates that roughly 70% of people turning 65 today will need some form of long-term care during their lifetime, with women averaging 3.7 years of need and men averaging 2.2 years. For early retirees, the horizon is even longer — a tech worker who retires at 45 may spend 40+ years in retirement before care needs emerge, during which time LTC costs will have inflated substantially. Failing to plan for this is not a conservative position; it is an optimistic bet against statistics.
What Long-Term Care Actually Covers
Long-term care is delivered across a spectrum of settings:
- Home care: A home health aide or personal care assistant comes to the home to help with daily activities. This is the most preferred setting for most people and can range from a few hours per day to 24-hour live-in care.
- Adult day programs: Structured daytime care at a facility, allowing a family caregiver to work or rest. Lower cost than residential care.
- Assisted living facility (ALF): Residential care for people who need help with daily activities but not round-the-clock nursing supervision. Typically includes meals, housekeeping, and personal care assistance in a private apartment setting.
- Memory care: A specialized type of assisted living for people with dementia or Alzheimer's, with secured units and staff trained in cognitive care. Generally costs 20–30% more than standard assisted living.
- Skilled nursing facility (nursing home): The highest level of non-hospital residential care, providing 24-hour nursing supervision. Required when medical needs exceed what assisted living can manage.
The Real Cost of Long-Term Care
LTC costs are large, inflation-sensitive, and geographically variable. National median costs in 2024:
- Home health aide (full-time, 44 hours/week): approximately $62,000–$75,000 per year
- Assisted living facility: approximately $5,000–$6,500 per month ($60,000–$78,000 per year)
- Memory care facility: approximately $6,000–$9,000 per month
- Nursing home, private room: approximately $9,000–$10,500 per month ($108,000–$126,000 per year)
In high-cost metropolitan areas — the Bay Area, New York City, Boston — these figures run 50–100% higher. A private nursing home room in San Francisco can exceed $200,000 per year. LTC costs have historically inflated at 3–5% annually, faster than general CPI. A cost of $100,000 per year today becomes $180,000–$220,000 in 20 years at that rate.
For a married couple where both spouses eventually need care — statistically common — the aggregate lifetime LTC cost can easily exceed $500,000 and in severe cases approach $1,000,000 or more. This is large enough to materially threaten a retirement portfolio that looked fully funded on paper.
What Medicare Does NOT Cover
The single most widespread and costly misconception in LTC planning is that Medicare will pay for it. It will not — at least not in any meaningful long-term way.
Medicare covers skilled nursing care only after a qualifying hospital stay of at least three days, and only for a limited time: fully covered for days 1–20, a daily copay ($204/day in 2025) for days 21–100, and nothing after day 100. Medicare covers this only when skilled nursing is medically necessary — physical therapy after surgery, wound care, IV medications. The moment care transitions from skilled rehabilitation to custodial maintenance (helping someone bathe because they can no longer do it independently), Medicare coverage ends.
Medicare also covers some home health services, but only when the patient is homebound and requires skilled nursing or therapy. Ongoing personal care assistance from a home health aide — the most common form of long-term care — is not covered once skilled need ends. The assumption that Medicare will fund years of assisted living or in-home care is simply wrong.
Medicaid: The Safety Net With a Steep Price
Medicaid does cover long-term care, including nursing home care and, in many states, home and community-based care. It is the primary payer for nursing home care in America. But accessing Medicaid for LTC requires meeting both income and asset limits — effectively depleting most of your savings first.
To qualify for Medicaid LTC benefits, a single individual must typically reduce countable assets to $2,000 or less. A married couple receives more protection — the community spouse (the one not needing care) can retain a protected amount of assets, but this Community Spouse Resource Allowance (CSRA) caps out at approximately $154,000 in most states. All assets above the limit must be spent on care before Medicaid begins paying.
This spend-down process means that a tech worker who retired with $3,000,000 and needs nursing home care at age 80 would spend down from $3,000,000 to the Medicaid limit before Medicaid contributes a dollar — potentially exhausting most of the portfolio and leaving a surviving spouse with dramatically reduced resources. Relying on Medicaid as an LTC plan is not a financial strategy; it is the absence of one.
Additionally, Medicaid LTC benefits typically cover nursing home care in facilities that accept Medicaid — which often have lower staff-to-patient ratios and fewer amenities than private-pay facilities. Choice of facility is significantly constrained once on Medicaid.
Long-Term Care Insurance
LTC insurance is specifically designed to cover custodial care costs, paying a daily or monthly benefit when the policyholder meets the benefit trigger — typically inability to perform two or more activities of daily living (ADLs) or severe cognitive impairment.
Traditional LTC Insurance
Traditional standalone LTC policies pay a defined daily or monthly benefit (e.g., $200/day, $6,000/month) for a specified benefit period (2 years, 5 years, unlimited). Key policy features:
- Elimination period: The waiting period before benefits begin — typically 30, 60, or 90 days. A 90-day elimination period means you pay the first 90 days of care out of pocket before insurance starts. Longer elimination periods reduce premiums.
- Inflation protection: Critical given LTC cost inflation. A 3% compound inflation rider increases the daily benefit by 3% per year, so a $200/day benefit purchased at 55 becomes $322/day by age 75. Without inflation protection, a benefit that seems adequate today may be inadequate in 20 years.
- Benefit period: How long the insurance pays. A 3-year benefit period covers average needs for most people; a 5-year period adds significant protection for longer care needs. Unlimited benefit periods are expensive but available.
Traditional LTC insurance has a significant drawback: use-it-or-lose-it. If you stay healthy and never need care, you receive nothing back from years of premiums — similar to auto insurance. Additionally, insurers have significantly raised premiums on existing policyholders in recent years as claims experience exceeded projections, leading some insurers to exit the market. Premiums can increase after purchase, which creates budget uncertainty in retirement.
Hybrid LTC Insurance (Life Insurance + LTC Rider)
Hybrid policies combine permanent life insurance (typically whole or universal life) with a long-term care benefit rider. If you need LTC, the policy pays benefits; if you die without using the LTC benefit, the remaining death benefit passes to heirs. The "use-it-or-lose-it" problem of traditional LTC is largely eliminated — your premium is not wasted if you stay healthy.
Hybrid policies are typically funded with a single lump-sum premium or over 10 years, rather than recurring annual premiums indefinitely. This makes budgeting more predictable. They have become the dominant form of new LTC planning in recent years as traditional LTC insurers have exited the market.
The trade-off: hybrid policies are generally more expensive for the pure LTC coverage provided, and the investment return inside the life insurance component is modest. For someone who could otherwise invest the premium in equities, a hybrid policy may deliver lower expected return — but it provides certainty and eliminates the risk of premium increases or policy lapse.
Tax Treatment of Long-Term Care
LTC Insurance Premium Deductibility
Premiums paid for a tax-qualified LTC insurance policy are deductible as a medical expense, subject to an age-based limit and the 7.5% AGI floor for medical deductions. The age-based deductible limits for 2025 (adjusted for inflation annually):
- Age 40 or under: $470
- Age 41–50: $880
- Age 51–60: $1,760
- Age 61–70: $4,710
- Age 71 and older: $5,880
Self-employed individuals can deduct LTC premiums up to these limits directly from gross income (on Schedule 1) without needing to itemize and without the 7.5% AGI floor — a meaningful advantage. S-corp owners can have the corporation pay premiums and include them in W-2 wages, then deduct them as self-employed health insurance.
HSA Funds for LTC Premiums
Health Savings Account (HSA) funds can be used to pay LTC insurance premiums tax-free, up to the same age-based limits above. This makes an HSA one of the most tax-efficient ways to fund LTC premiums — contributions are pre-tax, growth is tax-free, and qualified withdrawals (including LTC premiums) are tax-free. For early retirees who have accumulated a large HSA balance, using it to pay LTC premiums is an excellent tax-efficient deployment of those funds.
Benefits Received Are Generally Tax-Free
Benefits received from a tax-qualified LTC insurance policy are generally excludable from income up to the greater of actual LTC costs incurred or the IRS per diem limit ($420/day in 2025). Most people receiving LTC benefits are below this limit, meaning the insurance proceeds are effectively tax-free income.
LTC Planning for Early Retirees
Early retirees face a unique LTC challenge: they may go 30–50 years before needing care, during which time LTC costs will inflate substantially, but they also have decades of portfolio compounding available to self-fund. The key questions are:
- Self-fund vs. insure: A portfolio of $5,000,000+ with disciplined withdrawal rates may be able to absorb even worst-case LTC costs without insurance. A portfolio of $1,500,000 could be significantly depleted by a long care event — insurance transfers this risk. The break-even depends on portfolio size, expected returns, and risk tolerance for catastrophic care scenarios.
- When to buy LTC insurance: Premiums are lower the younger you purchase, but paying premiums for decades before you need care is expensive. Many planners recommend purchasing in the mid-50s — old enough to have reasonable premium predictability, young enough to pass underwriting and lock in reasonable rates before health issues emerge. Waiting until 65 or later significantly increases both premium costs and the risk of being declined due to health.
- Protecting the community spouse: For married couples, LTC planning is fundamentally about protecting the healthy spouse's financial security when one partner needs care. A long nursing home stay for one spouse can deplete the joint portfolio and leave the surviving spouse with inadequate resources for their own retirement. LTC insurance or a robust self-funding reserve specifically sized for this scenario should be part of every married couple's plan.
Common Mistakes in Long-Term Care Planning
1. Assuming Medicare Covers It
The most dangerous mistake. Medicare covers up to 100 days of skilled nursing care after a qualifying hospital stay and nothing beyond that for custodial care. Most LTC needs — years of assisted living, in-home aide support, memory care — are not covered by Medicare at all. Building a retirement plan that assumes Medicare handles LTC is building on a false foundation.
2. Waiting Until It's Too Late to Qualify
LTC insurance requires medical underwriting. If you wait until you have significant health issues — the early stages of cognitive decline, a recent stroke, advanced diabetes, severe obesity — you may be declined entirely or face premiums so high the policy is uneconomical. The window for purchasing LTC insurance at reasonable rates and qualifying health is roughly ages 50–65. Waiting to "see if you need it" is a strategy that can result in no coverage being available when you realize you do.
3. Buying Inadequate Coverage
Many people purchase LTC insurance with low daily benefits, no inflation protection, or short benefit periods to keep premiums affordable — and end up with a policy that covers a fraction of actual costs when care is needed. A $150/day benefit purchased without inflation protection in 2005 covered roughly a semi-private nursing room in many markets. That same $150/day in 2025 barely covers a few hours of home care aide time. If you buy LTC insurance, the inflation protection rider is non-optional for anyone more than a few years from likely need.
4. Not Having Any Plan at All
The most common mistake is simply not addressing LTC in the financial plan. Many people — including disciplined savers who have meticulously planned every other aspect of retirement — have no answer to the question "what happens if one of us needs nursing home care for five years?" The absence of a plan does not make the risk disappear; it just means the financial damage, when it occurs, is entirely unmitigated.
5. Underestimating the Caregiver Burden on Family
Without a formal LTC plan, the default is often that family members — typically a spouse or adult children — become unpaid caregivers. The financial and personal cost of family caregiving is enormous: lost income from reduced work hours or career interruption, physical and emotional burnout, relationship strain. For tech workers whose children may themselves be in demanding careers, assuming family will "figure it out" imposes a significant burden that a proper LTC plan would eliminate or reduce. Having the conversation explicitly and building a plan that does not assume family caregiving as the default is an act of consideration for the people you love.
6. Conflating LTC With Health Insurance
ACA marketplace health insurance, employer health insurance, and Medicare all cover medical care — doctor visits, hospital stays, surgeries, prescription drugs. None of them cover custodial long-term care. This distinction confuses many early retirees who carefully plan their ACA coverage during the gap years before Medicare eligibility, believing health insurance solves the care cost problem. It does not. Health insurance and LTC insurance solve completely different risks.
7. Treating Medicaid as a Backup Plan
Some people consciously decide to spend down assets and rely on Medicaid if they need nursing home care. This is a legitimate choice for those with modest assets, but for tech workers with substantial portfolios, it has serious consequences: the spend-down requirement can deprive a surviving spouse of financial security, Medicaid facility selection is constrained, and the assets you intended to leave to heirs or charity are consumed by care costs before Medicaid begins. Medicaid is a safety net for people who have no other option — planning to use it deliberately is planning to impoverish yourself first.
Frequently Asked Questions
Build Long-Term Care Into Your Retirement Plan
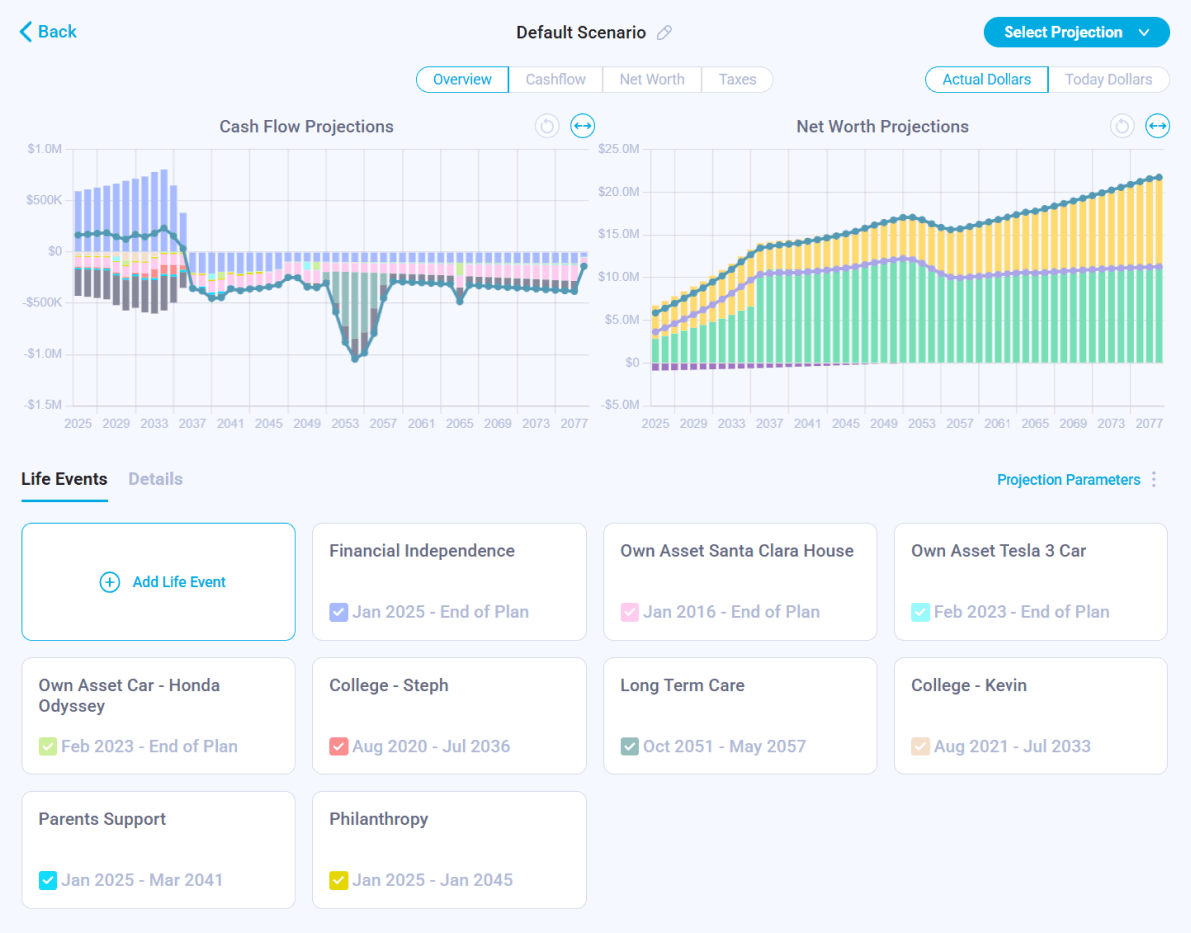
Nauma models long-term care costs alongside your portfolio projections — showing how a care event affects retirement sustainability and helping you decide between self-funding, insurance, or a hybrid approach.
Get Started for Free